| No. 70 Music & Medicine | |
|
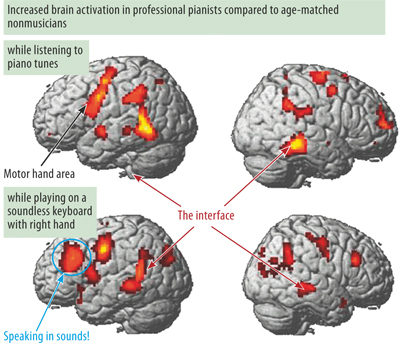
Performing music at a professional level is perhaps one of the most complex of human accomplishments. As a sensory stimulus, music is both exceedingly intricate and structured along several dimensions. Moreover, making music requires the integration of multimodal sensory and motor information together with precise monitoring of motor performance via auditory feedback. In the context of western classical music, musicians must reproduce highly controlled movements almost perfectly and with high reliability. These specialized sensory-motor skills require extensive training periods over many years, starting in early infancy and passing through stages of increasing physical and strategic complexity. Sensory-motor skills in musicians are usually automated by many repetitions. Aural skills on the other hand are typically refined through a broad variety of listening experiences. Both types of skill, however, are not represented in isolated brain areas but depend on the multiple connections and interactions established during training within and between different regions of the brain. Musicians can learn new works and improve their skills over many years because the central nervous system (CNS) is able to adapt to changing environmental conditions and newly imposed tasks during its entire life span, a phenomenon that is referred to as plasticity. In music, learning through experience and training is accompanied by remarkable brain adaptations, which are reflected not only in modifications of the brain’s neuronal networks through enhanced neuronal connectivity but also in its overall gross anatomy. Music practice enhances myelination, gray matter growth and fiber formation of brain structures involved in the specific musical task [1]. There are two main reasons why researchers believe that these effects on brain plasticity are more pronounced in instrumental music performers than in those undertaking other skilled activities. First, musical training usually starts very early, sometimes before age six, when the adaptability of the CNS is highest. Second, musical activities are strongly linked to positive emotions, which are known to enhance plastic adaptations. This review will focus on new insights into brain mechanisms involved in musical performance and practice. First, I will demonstrate changes in brain networks and structures accompanying musical achievements. I will then briefly comment on the neural foundations of training strategies such as mental and observational practice. After addressing the effect of music training on general cognitive abilities, I will conclude with a discussion of effects related to maladaptive changes of brain networks, resulting in movement disorders such as musician’s dystonia. Wiring the Brain: Music Making as a Sensory-Motor Integration Task As mentioned above, performance-based music making relies primarily on a highly developed integration of auditory and motor abilities. In addition, feedback in the somatosensory system (that is, the receptors and processors related to e.g. touch and body position) constitutes another basis of high-level performance. Especially important here is the kinesthetic sense, which enables control and feedback of muscle and tendon tension as well as joint positions which allow continuous monitoring of finger, hand or lip position within the frameworks of body and instrument coordinates (e.g. the keyboard, the mouthpiece). One special quality of musicianship therefore is the strong coupling of sensorimotor and auditory processing. Practicing an instrument involves assembling, storing and constantly improving complex sensorimotor programs through prolonged and repeated execution of motor patterns under controlled monitoring by the auditory system. Many professional pianists for example report that their fingers move more or less automatically when they are listening to piano music played by a colleague. A cross-sectional experiment undertaken with professional pianists revealed strong linkages between auditory and sensory-motor cortical regions developed over many years of practice. Using functional magnetic resonance imaging, subjects were asked to listen to simple piano tunes without moving their fingers or any other body part. Figure 1 shows the increased neuronal activation of professional pianists in comparison to nonmusicians. There is an impressive activation of the motor cortex, demonstrating subconscious or automated auditory-motor coactivation.
Furthermore, in a longitudinal study, it was possible to follow the formation of such neuronal multisensory connections during piano training by beginning pianists. Nonmusicians, who had never played an instrument before, were trained on a computer piano twice a week over a period of five weeks. They listened to short piano melodies of three-second duration played in a five-tone range, and were then required, after a brief pause, to replay the melodies as accurately as possible with their right hand. After 20 minutes of training, first signs of increased neuronal coupling between auditory and motor brain regions were observable. After five weeks, listening to piano tunes produced additional activity in the central and left sensorimotor regions. Playing on a mute (soundless) keyboard produced additional activity in the auditory regions of both temporal lobes [3]. This experiment impressively demonstrates how dynamically brain adaptations accompany these multiple sensorimotor learning processes. Activation of motor corepresentations can occur in trained pianists not only by listening to piano tunes, but also by observing a pianist’s finger movements on a video. The brain mechanisms of such learning through observation have been clarified in recent years. When monkeys observed the actions of other monkeys, for example grasping peanuts, exactly the same brain areas were active as if the observing animals were performing the observed action themselves. Additionally, a region in the parietal lobe of the observing monkeys was activated, which is believed to represent the knowledge that ‘it is not me who is performing the action.’ Quite appropriately, this neuronal network has been termed a ‘mirror neuron network.’ When trained pianists are observing video sequences of a moving hand at the piano, the motor hand area in the primary motor cortex, and secondary auditory cortices in the temporal lobe and the cerebellum are activated, convincing evidence for such a mirror system in humans. What this means for musical practice is that careful demonstration at the instrument may enhance learning. Practicing through listening and/or observation can be considered special cases of mental training. Narrowly defined, mental training is understood as the vivid imagination of movement sequences without physically performing them. As with the observation of actions, by and large when an action is imagined, the same brain regions are active as if the imagined action were actually being performed; that is, the primary motor cortex, the supplementary motor cortex and the cerebellum. In a study investigating mental training of finger movement sequences of different complexities, brain activation increased with the degree of difficulty of the imagined motor task. Furthermore, when continuing mental practice over a period of several days, the involved brain regions showed plastic adaptations. Although these adaptations were less dramatic than if the motor tasks had been practiced physically, mental training produced a clear improvement in task performance as assessed in finger-tapping tests. Plasticity of Sensory Motor Systems: Musicians’ Brains Are Different During the past decade, brain imaging has provided important insights into the enormous capacity of the human brain to adapt to complex demands. Brain plasticity is best observed in complex tasks with high behavioral relevance for the individual, i.e. that cause strong emotional and motivational activation. Plastic changes are more pronounced in situations where the task or activity has been developed early in life and whose performance is intense. Obviously, the continued activities of accomplished musicians provide the ideal prerequisites for brain plasticity, and it is not astonishing that the most dramatic brain plasticity effects have been demonstrated in professional musicians [1]. Our understanding of the molecular and cellular mechanisms underlying these adaptations is far from complete. Brain plasticity may occur on different time axes. For example, the efficiency and size of synapses may be modified in a time window of seconds to minutes, while the growth of new synapses and dendrites may require hours to days. An increase in gray matter density, which mainly reflects an enlargement of neurons, needs at least several weeks. White matter density also increases in response to musical training. This effect is primarily due to an enlargement of myelin cells. Myelin cells, wrapped around the nerve fibers (axons), contribute to the velocity of the electrical impulses traveling along the nerve fiber tracts. Under conditions requiring rapid information transfer and high temporal precision, these myelin cells grow and nerve conduction velocity increases. Finally, brain regions involved in specific tasks may also be enlarged after long-term training due to the growth of structures supporting nerve function, for example, the blood vessels that are necessary for transport of oxygen and glucose to sustain neuronal activity. Comparison of the brain anatomy of skilled musicians with that of nonmusicians shows that prolonged instrumental practice leads to an enlargement of the hand area in the motor cortex and to an increase in gray matter density corresponding to more and/or larger neurons [4]. These adaptations appear to be particularly prominent in all instrumentalists who have started to play prior to the age of ten and correlate positively with cumulative practice time. Furthermore, in professional musicians, the anatomical difference between the larger, dominant (mostly right) hand area and the smaller, nondominant (left) hand area is less pronounced than in nonmusicians. These results suggest that functional adaptation of the gross structure of the brain occurs during training at an early age. The size of the corpus callosum also responds to such specialization. Professional pianists and violinists, and especially those who started to play prior to the age of seven, tend to have a larger anterior (front) portion of this structure [5]. Since this part of the corpus callosum contains fibers from the motor and supplementary motor areas, it seems plausible to assume that the high demands on coordination between the two hands and the rapid exchange of information may either stimulate nerve fiber growth – the myelination of nerve fibers that determines the velocity of nerve conduction – or prevent the physiological loss of nerve tissue during aging. It is not only motor areas, however, that are subject to anatomical adaptation. With magnetoencephalography it is possible to monitor the number of nerve cells involved in the processing of auditory or somatosensory stimuli. Professional violinists have been shown to possess enlarged sensory areas corresponding to the index through to the small (second to fifth) fingers of the left hand [6], while their left thumb representation is no different from that of nonmusicians. Again, these effects are most pronounced in violinists who started their instrumental training prior to the age of ten. In summary, when training starts at an early age (before about seven years), these plastic adaptations of the nervous system affect brain anatomy by enlarging the brain structures that are involved in different types of musical skill. When training starts later, it modifies brain organization by rewiring neuronal webs and involving adjacent nerve cells to contribute to the required tasks. These changes result in enlarged cortical representations of, for example, specific fingers or sounds within existing brain structures. The Impact of Musical Training on General Cognitive Skills It has long been assumed that an increase in brain connectivity or in gray matter density can improve general cognitive abilities. Typically, this is investigated with intervention studies assessing the effect of music lessons on performance in other cognitive domains. For example, in Montreal (Canada) between 1994 and 1997, Eugenia Costa-Giomi compared intelligence quotients (IQs) in children with and without piano lessons. Sixty-seven 9-year-old children from a rather poor social stratum were given weekly piano lessons for three years; the control group of 50 children had no piano lessons. At the beginning of the study all the children showed the same IQ for language, spatial and mathematical performance. After two years, the piano students were ahead in all three tested IQ domains; however, after three years, the children in the control group had caught up [7]. Similar results have been obtained in more recent studies. In an intervention study led by Schellenberg, 144 6-year-old children were given piano lessons, singing lessons, drama lessons or none of these for a period of 36 weeks. After these nine months, the IQ values for the children with piano and singing lessons were 3–3.5 higher than for the other children [8]. Such effects of music lessons on cognition are apparently not restricted to children. Bugos and colleagues [9] gave piano lessons for six months to 20 senior citizens aged between 60 and 85 years and compared their cognitive skills with those of 18 similar elderly people. After the piano lessons, the piano group showed significant improvements in memory performance, working memory, planning memory and strategy management. Perhaps the most convincing transfer effects can be found in the domain known as ‘emotional competence.’ Music education, for example, improves the ability to decode affective states in spoken language. Apollo’s Curse: Focal Dystonia There is a dark side to the increasing specialization and prolonged training of musicians, namely loss of control and degradation of skilled hand movements, a disorder referred to as musician’s cramp or focal dystonia (Fig. 2). The first historical record, from 1830, appears in the diaries of the ambitious pianist and composer Robert Schumann [10]. As was probably the case for Schumann, prolonged practice and pain syndromes due to overuse can precipitate dystonia, which is developed by about 1% of professional musicians and in many cases ends their career. Subtle loss of control in fast passages, finger curling (Fig. 2), lack of precision in forked fingerings in woodwind players, irregularity of trills, fingers sticking on the keys, involuntary flexion of the bowing thumb in string instrument players and impairment of control of the embouchure in woodwind and brass players in certain registers are the various symptoms that can mark the beginning of the disorder. At this stage, most musicians believe that the reduced precision of their movements is due to a technical problem. As a consequence, they intensify their efforts, but this often only exacerbates the problem.
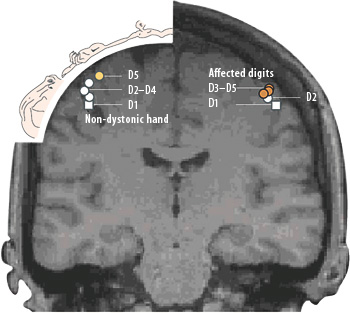
Males, classical musicians of a younger age and instrumentalists such as guitarists, pianists and woodwind players are among the most commonly affected by focal dystonia. The majority of patients are soloists and often have a perfectionist, control-type personality. About 20% of such patients report a history of chronic pain syndromes or overuse injury. Preventing these musicians from developing chronic overuse and tendinitis will most probably prevent them from developing focal dystonia [11]. However, once focal dystonia is established, the cure of the pain syndrome will generally not eliminate the pathological movement pattern. The etiology of focal hand dystonia is not completely understood, but is probably multifactorial. Most studies of focal dystonia reveal abnormalities in three main areas: (a) reduced inhibition in the motor system at cortical, subcortical and spinal levels, (b) reduced sensory perception and integration and (c) impaired sensory-motor integration. The latter changes are mainly believed to originate from dysfunctional brain plasticity. In patients with focal dystonia, there is growing evidence for abnormal cortical processing of sensory information as well as degraded representation of motor functions. A study with trained monkeys demonstrated that chronic overuse and repetitive strain injury in highly stereotyped movements can actively degrade the cortical representation of the somatosensory information that guides the fine motor hand movements in primates. A similar degradation of sensory feedback information and concurrent fusion of the digital representations in the somatosensory cortex was confirmed in a brain activation study conducted in musicians with focal dystonia. Compared to healthy musicians, those with dystonia showed a fusion of the digital representations in the somatosensory cortex, reflected in the decreased distance between the representation of the index finger and the little finger (Fig. 3). Such a fusion and blurring of receptive fields of the digits may well result in a loss of control, since skilled motor actions are necessarily bound to intact somatosensory feedback input. Since these musicians had no history of chronic pain, additional factors such as a genetic predisposition appear to play an important role in the development of focal dystonia [12].
Unfortunately, there is no simple cure for the condition. Retraining may be successful in a minority of cases, but usually requires several years. Symptomatic treatment with temporary weakening of the cramping muscles by injecting botulinum toxin has proven helpful in other cases; however, since the injections need to be applied regularly every three to five months during the professional career, it presents no solution for young patients. Thus, the challenge is to prevent young musicians developing such a disorder. Reasonable practice schedules, economic technique, prevention of overuse and pain, mental practice, avoidance of exaggerated perfectionism, and psychological support with respect to self-confidence are the components of such a prevention program. Conclusion Musical performance is an excellent model to study the effects of neuroplasticity in the auditory and the sensory-motor domains. It seems to be one of the most powerful stimuli to drive plastic changes in the CNS. Future studies with professional musicians may allow us to differentiate the contributions of experience and training from those of genetic predisposition. Investigations of focal dystonia, meanwhile, may help to delineate the effects of dysfunctional plasticity due to overuse. We are still, though, some way from the answers to one important question posed by the findings that have been discussed here. Music elicits strong emotional (and intellectual) responses. For humans, such responses are as essential to high-quality performance as to the reception of music and they are accompanied by strong activations of the limbic system – a network of brain centers at the inner border of the cortex – which is involved in reward, emotion and motivation. Much more research is required to show whether and how it is activity in areas of this network that mediates the strong and dynamic neuroplastic adaptations seen in performing musicians.
 Eckart Altenmüller (b. 1955) holds an MA in classical flute and an MD and PhD in neurology and neurophysiology. In 1994 he became Chair and Director of the Institute of Music Physiology and Musicians’ Medicine, Hannover. His research focuses on the neurobiology of emotions and movement disorders in musicians as well as motor and sensory learning. Since 2005 he has been President of the German Society of Music Physiology and Musicians’ Medicine and a member of the Göttingen Academy of Sciences.
Prof. Dr. med. Eckart Altenmüller MD, MA, PhD Director Institute of Music Physiology and Musicians'Medicine (IMMM) University of Music and Drama Hanover Hohenzollernstrasse 47 D-30161 Hannover Germany altenmueller@hmt-hannover.de Homepage |
|||||||||||||||||||||||||||||||||