| No. 67 Skin |
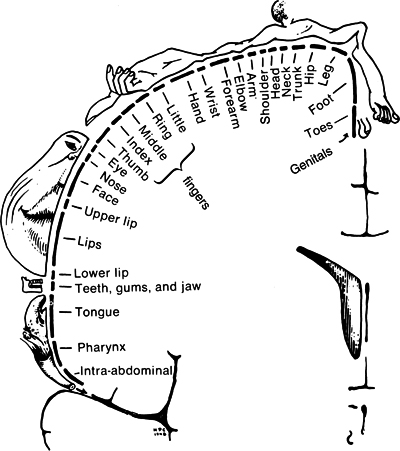
Touch appears to be important for survival and well-being in all species with this sense. For example, rat pups do not survive without their mothers' tongue-licking touch, and mother goats abandon their young if the baby goat is touched by another animal or a human. Monkeys become extremely aggressive when they are touch deprived. The power of touch in young children was demonstrated in a study in which one group of preschool children in a pediatric ward was given only verbal comfort when they showed distress, while the other was given simultaneous verbal and tactile comfort, including holding, patting, rocking, stroking and being offered a pacifier. Only 7 of the 40 verbal comforts succeeded in quieting the children, but 53 of the 60 tactile-verbal comforts were successful [2]. Messages to the brain The term touch includes several tactile senses: pressure, pain, temperature and muscle movement. Many sensory receptors at different levels in the skin are responsible for conveying the nerve signals from thermal, mechanical, chemical and electrical stimuli. Meissner's corpuscles, located between the epidermis and the dermis on the hairless parts of the body – fingertips, palms, soles of the feet, tongue, sexual organs and so on – respond to the lightest form of stimulation. The pacinian corpuscles, located near the joints and deep tissues and in the genitals and mammary glands, respond to pressure, vibrations and high-frequency sounds. Merkel's disks, located just beneath the skin, respond to constant pressure. Ruffini endings, located deep in skin, can also register pressure and temperature. Information from touch-sensitive nerve cells ultimately crosses the sensory cortex to the opposite side of the brain where it is processed. The amount of space needed by the cortex is related not to the size of the body part but to the nerve density: areas with more nerve endings, such as fingertips, lips and genitals, require more space in the cortex than the back, which has fewer nerve endings (fig. 1) [3]. Cortical nerve cells may be highly specialized: some, for example, will respond only to stroking the surface of a body part in one single direction, others to stroking at a specific frequency. Those areas of the body with a high density of nerve endings are also most sensitive to pain.
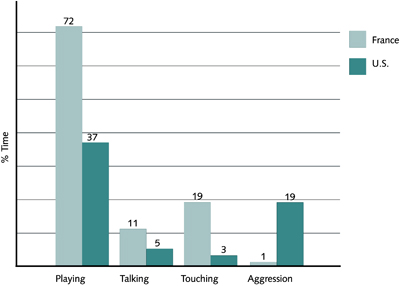
Touch in culture Some cultures touch more than others. For example, in African cultures, babies are passed from person to person for many years, and the French are known to touch people more than Americans and certainly more than the British. People touch each other more during the preschool years than across the lifespan. In a recent study we noted, for example, that French mothers touched their preschoolers more at McDonald's in Paris than American mothers did at McDonald's in Miami (fig. 2) [4]. The French children, in turn, were less aggressive toward each other on the playground. French teenagers touched each other more at McDonald's in Paris while teenagers touched themselves (like self-hugging and playing with their hair) more at McDonald's in Miami. The French teenagers were also less aggressive with each other than were the American adolescents.
Young children depend on touch for learning about the world including the qualities of temperature, texture, shape, softness, sharpness, elasticity and resilience. Children also learn safety from touch such as avoiding stoves, sharp objects or frostbite, and they may learn how to write through touch if given hand-over-hand assistance in handwriting classes. Touch is not only critical for growth, development, communication and learning but also serves for comfort, reassurance and self-esteem. The first emotional bonds are based on physical contact, and they form the foundation for emotional and intellectual development (fig. 3). Despite these critical functions of touch, most children in the United States are socialized from a very early age to limited touch. They are punished for touching their own body parts and learn not to touch the bodies of others. They learn by adolescence that they should be cautious about physical intimacy. As adults they may talk about touch in many personal and sentimental ways, but in America's litigious landscape, they have become afraid of touching others because of potential lawsuits.
In the USA, mothers spend about 60% of their interaction time touching their infants. Soothing stimulation by parents is replaced by peer play (rough-and-tumble play at the preschool stage and contact sports during high school). But as children grow older, physical contact from parents becomes more taboo. As children reach high school, they receive about half the touch that they did in primary school. The nature of the touching also changes: there is more shoulder-to-shoulder and elbow-to-elbow rather than hand contact. The American adolescent typically treats family members as if they had some dread disease. Given the American touch taboos it is not surprising that touch-deprived adolescents might be drawn to touch-dancing, skinny-dipping, nude beaches, long showers, sunbathing marathons, applying lots of makeup and peer backrubs. These adolescent touch habits seem to have evolved at around the same time that schools mandated that teachers could no longer hug or touch children. Some go so far as to say that touch is our strongest contact. In the words of Saul Schanberg: “Touch is ten times stronger than verbal or emotional contact, and it affects damned near everything we do. No other sense can arouse you like touch. We always knew that, but we never realized that it had a biological basis. If touch did not feel good, there would be no species, parenthood or survival. The mother would not touch her baby in the right way unless the mother felt pleasure in doing it. If we did not like the feel of touching and patting one another we would not have had sex. Those animals that did more touching instinctively produced offspring, which survived and had more energy, and so passed on their tendency to touch which became even stronger. We forget that touch is not only basic to our species but the key to it.” [5]. Dr Schanberg has isolated a gene for growth that can only be ”turned-on“ by touch. In his rat model, the pups deprived of touch had significantly reduced growth hormone resulting in zero growth [6]. Touch in health The'laying-on of hands' has a long tradition, and the Ebers Papyrus dated to 1553 BC provides evidence of the early practice of healing by touch. In Hippocrates' Greece, around 400 BC, there were hand healers called kheirourgos. This is the origin of the word 'surgeon,' though the Greeks used the palm and their fingers, not surgical methods, to heal. One of the most famous Roman healers, Galen (130 AD), used massage as a medical treatment. There is ample evidence for healing via the hands throughout the Bible and, in the West, the laying-on of hands continued right through to the 18th century. But then it fell out of favor, possibly because of an increase in sexual taboos as well as the development of drugs and treatment technologies that have dramatically changed the field of medicine. Nevertheless, many of the touch therapies which have been practiced for thousands of years throughout the world, together with Western massage techniques, are now gaining acceptance by both the general public, medical practitioners and, importantly, insurance companies. Touch therapies can be classified into three groups – energy methods, manipulative therapies and amalgams (combinations of the first two) – examples and brief descriptions are given in table 1.
Although the underlying mechanisms for the effects of touch are unknown, positive effects have been noted for many growth, development and health phenomena as the following few examples will show. Children with autism are often described as being extremely sensitive and averse to touch. But they seem to accept massage, perhaps because it is predictable. In one study on preschool children with autism, their disruptive behavior in the classroom decreased and their ability to relate to their teachers increased after a 10-day period of massage. In a second study, parents massaged their autistic children every night. The children experienced the same benefits as in the first study, but their sleep also improved [7]. Massage could well be a fundamental way to reach out to these children who appear to reject adult attention and affection. Massage can also facilitate alertness. In a job-stress study, the staff and faculty of a medical school were massaged for 15 minutes a day for a month, during their lunch breaks. We recorded their EEG patterns before, during and after the massage sessions. Their alpha and beta wave levels decreased, while the theta increased, supporting the feelings of heightened awareness reported by the subjects. We also tested their performance on math computations. After massage, they took significantly less time to do the tasks and their accuracy increased [8]. Perhaps massage breaks should become as institutional as coffee breaks! Massage therapy has been noted to reduce pain in various pain syndromes. Children with juvenile rheumatoid arthritis experience chronic pain because their antiinflammatory medication is often only partially effective and they cannot be prescribed narcotics because of the risks of addiction. A 1-month study in which parents gave daily massages to their children with rheumatoid arthritis noted several positive effects: anxiety and stress levels decreased, as did the pain. There are several possible explanations for the reduced pain. The pressure nerves stimulated by the massage may transmit their messages faster to the brain than the pain receptors, thus closing a 'gate' and preventing the reception of the pain message. Another possibility is increased production of serotonin, which has both antidepressant and antipain properties. In addition, massage therapy has been noted to decrease symptoms in immune disorders such as asthma, diabetes and dermatitis and to enhance immune function, most particularly the production of natural killer cells that ward off cancer and viral cells [1]. We have noted in a recent study that moderate-pressure touch is necessary for these effects to occur. Moderate-pressure touch stimulates pressure receptors which in turn stimulate the vagus (one of the 12 cranial nerves) and increase vagal activity. This leads to a slowed heart rate and lower blood pressure, and the general behavioral effect is a relaxed, more attentive state. Other touch effects we have noted include a reduction in stress hormones (cortisol is a primary example), which could improve immune function, since cortisol normally kills natural killer cells. We also see an increase in activating neurotransmitters including serotonin and dopamine, and the alterations in EEG patterns which I have already mentioned. Infant massage Other than studying the physiological effects of touch and its critical importance for growth, development and health, my colleagues and I have been actively exploring ways to reintroduce touch into North American culture. One of the most promising ways may be teaching parents infant massage. Parents who are taught to massage their newborns continue to massage their children into adolescence. Infant massage training groups are now located in many parts of the United States, and the therapists claim that massage helps parent-infant bonding and warm, positive relationships, eases distress following painful procedures such as inoculations, reduces pain in teething and constipation, decreases colic and sleep problems and, importantly, reduces stress in the parents who are giving the massages. The techniques we teach are based on Indian infant massage, a daily routine beginning at birth, in which the infants are laid on their stomach on their mothers' outstretched legs. Each body part is stretched as warm water and soap are applied. The massage is quite rigorous, and afterwards the children are swaddled and sleep for prolonged periods. In one study, we taught depressed mothers to massage their infants, with the aim of both decreasing their depression and reducing the infants' associated distress behavior and disturbed sleep patterns. The mothers performed a 15-minute massage daily for 2 weeks. After 2 weeks, the infants were able to fall asleep faster, they slept longer and were less fussy, and the mothers played more easily with them. Studies have been undertaken in both Australia and the US on fathers' involvement in childcare. In the Australian study, fathers with first-born babies were given a 1-month training program in baby massage, including a bathing massage technique. In comparison with 'control' fathers, after 3 months, they showed greater involvement with their infants and the infants greeted their fathers with more eye contact, more smiling, more vocalization and reaching responses, and less avoidance behavior. In our American study, too, the fathers became more interactive with their infants after massaging them for 1 month (fig. 4).
One of the greatest deterrents to delivering massage to preterm infants is the cost of providing the massage. We have found that teaching 'grandparent' volunteers is a no-cost means to deliver massage therapy (fig. 5). And it's not only the children who benefit. In a study designed to measure massage effects on sexually and physically abused infants, we trained elderly volunteers to massage these children, and they themselves also received massage. The volunteers reported fewer depressive symptoms, an improved mood, and lower anxiety after both giving and receiving massage, and their stress hormone levels decreased. Their lifestyles showed other general improvements: they made more social contacts, fewer trips to the doctor's office and drank fewer cups of coffee, changes which probably helped to improve their sleep and self-esteem [9]. Interestingly, these improvements were greater after a month of giving infants massage than they were after a month of receiving massages.
Other ways that researchers and therapists have tried to introduce touch have included teaching 'good touch-bad touch' in classrooms and showing preschool and grade school-age children to give each other backrubs. These are small attempts in a still highly touch-inhibited western nation, but every effort adds to the knowledge base on the importance of touch for growth, development and health.
 Tiffany Field has been an active researcher in touch for the last 20 years and, in 1992, founded and currently directs the Touch Research Institutes at the University of Miami School of Medicine. She is also deeply involved in community research on child development, and is holder of the Chair Program and Past President of the International Society on Infant Studies (ICIS).
Tiffany Field, Ph.D Touch Research Institutes Univ. of Miami, School of Medicine P.O. Box 016820 Mailman Center for Child Development 1601 NW 12th Ave. 7th Floor S. 7037 Miami, FL 33101, USA Homepage: www.miami-edu/touch-research/ Email: tfield@med.miami.edu |
|||||||||||||||||||||||||||||||||||||||||||||||
| Close Window |